
Combination Cosmetic surgery in Non-Massive Weight Loss Patients:
(Multiple Site Aesthetic Surgery or Combined Cosmetic Surgery)
Combination cosmetic surgery is a term used to describe the performance of more than one cosmetic surgery procedure during the same operation. It refers to the procedures carried out at multiple sites or sites distant from each other. It does not refer to operations which are done in the same anatomical region or which complement each other. Examples of such exclusions are performance of a
-
combined breast lift & breast enlargement
-
brow lift at the same time as a face lift
-
a chin implant at the same time as a neck lift
-
a chin implant & a rhinoplasty
-
eyelid tucks & browlift
-
eyelid tucks & face lift
-
abdominoplasty & liposuction of the flanks
-
abdominoplasty & hernia repairs
-
thigh lifts & buttock lifts (posterior lower body lifts)
Cosmetic surgery patients frequently request multiple cosmetic procedures in a single operation due to time constraints and perceived financial benefits to them. However, combined cosmetic surgery is challenging and needs to be carefully planned for. Many such patients have often been refused combination cosmetic surgery procedures by other surgeons. Following the recent development of post-massive weight loss (PMWL) body contouring surgery, combined cosmetic surgery procedures have become commoner in that setting. There is however little information for patients and indeed in the medical literature for patients who don’t fall into this category and wish to have combined aesthetic procedures. Few surgeons offer this surgery because it is highly specialised and technically demaning. Professor Malata has considerable experience in performing combined cosmetic surgery in the non-PMWL population and his 10-year personal experience and outcomes have been presented at peer-reviewed scientific conferences (British Association of Plastic, Aesthetic and Reconstructive Surgeons’ Winter Meeting 2012).
Combined cosmetic surgery is well established in the rejuvenation of post-massive weight loss (PMWL) patients and in recent years it has given the impetus for such surgery to be performed in non-massive weight loss patients. It differs from PMWL combination surgery in that after massive weight loss the primary reason for the combination is anatomical proximity or areas which blend into each other or areas whose rejuvenation is complementary to each other. In such patients who have been left with excess loose tissues in different parts of the body the combinations are also frequently determined by practical issues such as the need to avoid turning the patient during surgery whilst on the operating table. In both groups of patients the individual patient choice of what areas of the body they want dealt with is also important in the decision making.
Principles of non-massive weight loss combination surgery:
Combined cosmetic surgery should not be entered into lightly and Professor Malata’s approach and philosophy is outlined below
Patient safety: Professor Malata’s primary concern is your safety and he will not undertake combination cosmetic surgery if, in his assessment, you have significant medical problems or your operation would be unduly long (more than 8 hours). Professor Malata seeks to minimise the length of surgery (and therefore the risks to you) hence he frequently performs only two cosmetic operations at the same time. Sometimes three cosmetic surgeries can be combined depending on their complexity and your overall medical condition and size. All these operations need to be performed in a regular hospital and not in a cosmetic clinic.
Need to avoid turning the patient intraoperatively: Professor Malata will often only perform surgeries in which the need for intraoperative turning of the patient on the table is minimized. This not only saves time but is also safer for the patient and makes the anaesthetic easier.
Monitoring: Sometimes because of the nature of the surgery a urinary catheter is required to monitor the urine output during a predictably long operation. Often this is removed the patient wakes up in the recovery room
Sequence: Synergistic operations are done in an order such as to avoid the 2nd operation undoing the “good work” of the 1st operation. A typical case in point is performing a tummy tuck before a breast lift or before a breast reduction. The tummy tuck pulls the breasts down and therefore the breast lift is usually performed after the breasts have been pulled down as much as possible by the tummy tuck.
Conversion to staged surgery: Professor Malata always informs his patients that very rarely it may be possible not to continue to the 2nd or 3rd planned operation because of time constraints, intraoperative difficulties or if the first operation takes much longer than originally planned. This is extremely rare.
Surgical Assistants: For such surgeries sometimes surgical assistants such as cosmetic surgery fellows, plastic surgery registrars, or specialist nurses to assist Professor Malata during your operation. They will, however, not be doing your operation but merely helping.
Surgical experience: It is important that your surgeon has experience and is trained in carrying out combination cosmetic surgery in order to optimise the outcome and keep risks to a minimum. This is because combined cosmetic surgery presents a number of challenges for all concerned; the patient and the carers.
Motivation for the patients:
-
Financial implications for patient; reduced overall costs
-
Time constraints for patient: one operation and one recovery period
-
Time away from work and family is reduced
-
Many patients have been turned down by other surgeons
-
Faster patient gratification
Problems for the patients:
-
Probable increased risks of complications and in particular infection risk
-
longer inpatient stay
-
longer recovery period,
-
Pain control/ lying comfortably/ attending to activities of daily living: for instance if both arms operated on, position in bed if back surgery (upper body lift) and abdominoplasty – extreme example.
Anesthetist challenges:
-
prolonged surgery but in practice not a major issue,
-
invasive monitoring may be required (central line, hourly urine output, fluid intake),
-
siting or location of intravenous lines for surgeries on all 4 limbs,
-
need for intraoperative turning (adequate staff, positioning, padding pressure points),
-
keeping patients warm when different parts are exposed or being operated on.
Problems for the surgeon:
-
Technical constraints
-
loss of momentum during position changes
-
surgeon fatigue
-
mental concentration on each surgery may be less
-
need for surgical assistance – presents challenges for single-handed practice
-
cost-inefficient on 2nd and subsequent procedures
Which combinations? This depends on what you are looking for but common cosmetic procedure combinations in Professor Malata’s practice are:
-
breast reduction & abdominoplasty
-
breast lift & abdominoplasty
-
breast augmentation & abdominoplasty
-
face lift & breast enlargement or breast lift
-
arm lifts & breast lifts
-
arm lifts & thigh lifts
-
abdominoplasty & thigh lifts
-
abdominoplasty & liposuction of thighs or calves
-
multiple site liposuction
-
labia minora reduction & non-implant breast surgery
Professor Malata’s experience: Over the 10-years (2002-2012), 97 patients underwent combined cosmetic surgery procedures in a single stage. Their ages ranged from 18-67 years and the male to female ratio was 1 male to 12 females. In terms of ethnic origin, two-thirds of the population were white caucasians, 13% black, 10% Asian, and 6% each for patients of Chinese and Mediterranean origin.
Four out of every five patients had 2 distinct procedures while the remaining one in five had three or more cosmetic operations at the same time. The commonest procedural combination was breast surgery and abdominoplasty (44/97) (two-thirds of which were breast reductions/breast lifts with a third being breast augmentations). The other combinations were breast cosmetic surgery and facial cosmetic procedures (18%), abdominoplasty with non-breast surgery (12%) and other multiple procedures (25%). For further details see Figure 1. Major complications needing re-operation or readmission to hospital were encountered in 5% of patients while 10% had minor wound healing problems that were successfully treated with dressing changes alone.
On analysing the commonest cosmetic procedural combination of breast cosmetic surgery with abdominoplasty it was found that its total theatre time was about one hour shorter than the sum of the times taked for the individual procedures. Specifically the combination reduced the operative time by about an hour –a practical factor in terms of scheduling the combined cosmetic surgery.
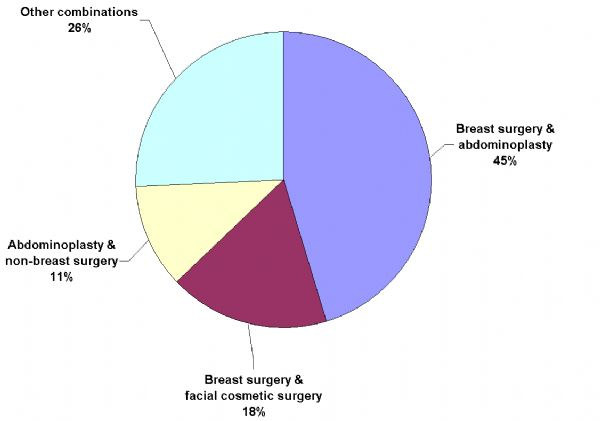
Figure 1: Pie chart showing combinations of aesthetic surgical procedures in Professor Malata’s practice.
Lessons from the study: Although it is assumed that combined cosmetic surgery leads to increased risks of complications, in practice the complication rate is similar to that reported for the individual cosmetic operations and lower than that in the massive weight loss patients. The pattern of combination cosmetic procedures requested by non-massive weight loss patients differs from post massive weight loss surgery. Needless to say combination surgery takes longer than single cosmetic procedures and potentially has the increased risks associated with prolonged anaesthesia. The recovery in terms of how long patients take to return to work and exercising is also longer. Patients should therefore be fully aware of the potential risks so that they can balance these against benefits of reduced cost and time away from work or family. The hospital stay may also be longer.
Conclusion: Multiple or combined cosmetic surgery procedures can be safely performed in patients requesting combination cosmetic surgery and hence patients should not be automatically turned down for combination cosmetic surgeries contrary to widespread UK practice.


